


Cancer Death Rates by Race/Ethnicity, U.S. 1968-2023
Plus a few notes on other cancer items and CDC data

Closing out “cancer week”, which has turned into a couple of weeks, let’s look at the high-level cancer age-adjusted death rate trend by race & ethnicity in the U.S.
Note: for those who are subscribed, a reader survey should have been emailed to you. This was a new tool substack just rolled out for us writers, so I’m unsure if this got deployed correctly.
Black vs. White, 1968-2023
Alas, the only two racial categories that are represented for the entire data period are White and Black (and this is not taking into account Hispanic origin).

Very broadly, the gap in mortality widened until the peak in the early 1990s, and then has been narrowing since then.
I did look at the spike in cancer death rates in 2021, to see if this was a spurious result (more on this in a bit). This does look to be a real increase in cancer deaths:
2019: 516,979
2020: 519,410
2021: 521,466
The population in total also was increasing in that period, in estimates, so the crude death rate was decreasing (slightly) from 2020 to 2021, but the age-adjusted death rate was increasing. In any case, it went back to decreasing in 2022 and 2023.
But back to the racial gap in age-adjusted death rates — in 1990, the gap was about 30%. But by 2023, the gap has shrunk to 9%. That is great improvement.
Some of the disparity is, I’m sure, due to differences in access to screening, not just treatment once cancer is found.
The overall shape of the cancer death rate curve, though, is hugely driven by smoking incidence. That may explain some of the disparities once I use more recent categories and data.
Race and Ethnicity, 1999-2023
Starting with 1999, we have more racial and ethnic categories to work with. I did look at Non-Hispanic White vs. White, but those weren’t too different. I just used the simplest categories for the next graph.

You can see that Hispanic and Asian groups have much lower age-adjusted death rates for cancer compared to White and Black.
In general, these groups have lower mortality rates and higher life expectancies in general U.S. population statistics.
There are a variety of reasons posited for that, but some major reasons can be dietary differences and lower smoking incidence:
US Cigarette Smoking Disparities by Race and Ethnicity — Keep Going and Going!
From 2011 to 2020, smoking prevalence significantly decreased from 9.9% to 8.0% among non-Hispanic Asian adults, from 19.4% to 14.4% among non-Hispanic Black adults, from 12.9% to 8.0% among Hispanic adults, and from 20.6% to 13.3% among non-Hispanic White adults.
I made my own graph from their data:

To be sure, it’s not a perfect correlation with what has occurred with cancer, but then, it generally takes decades for cancer to emerge and kill you, especially lung cancer, the most prominent deadly cancer.
On data anomalies
I mentioned in my last post on cancer death trends that the spike I was getting for older ages (ages 75+) for the year 2021 looked spurious, resulting from an odd trend in population estimates:
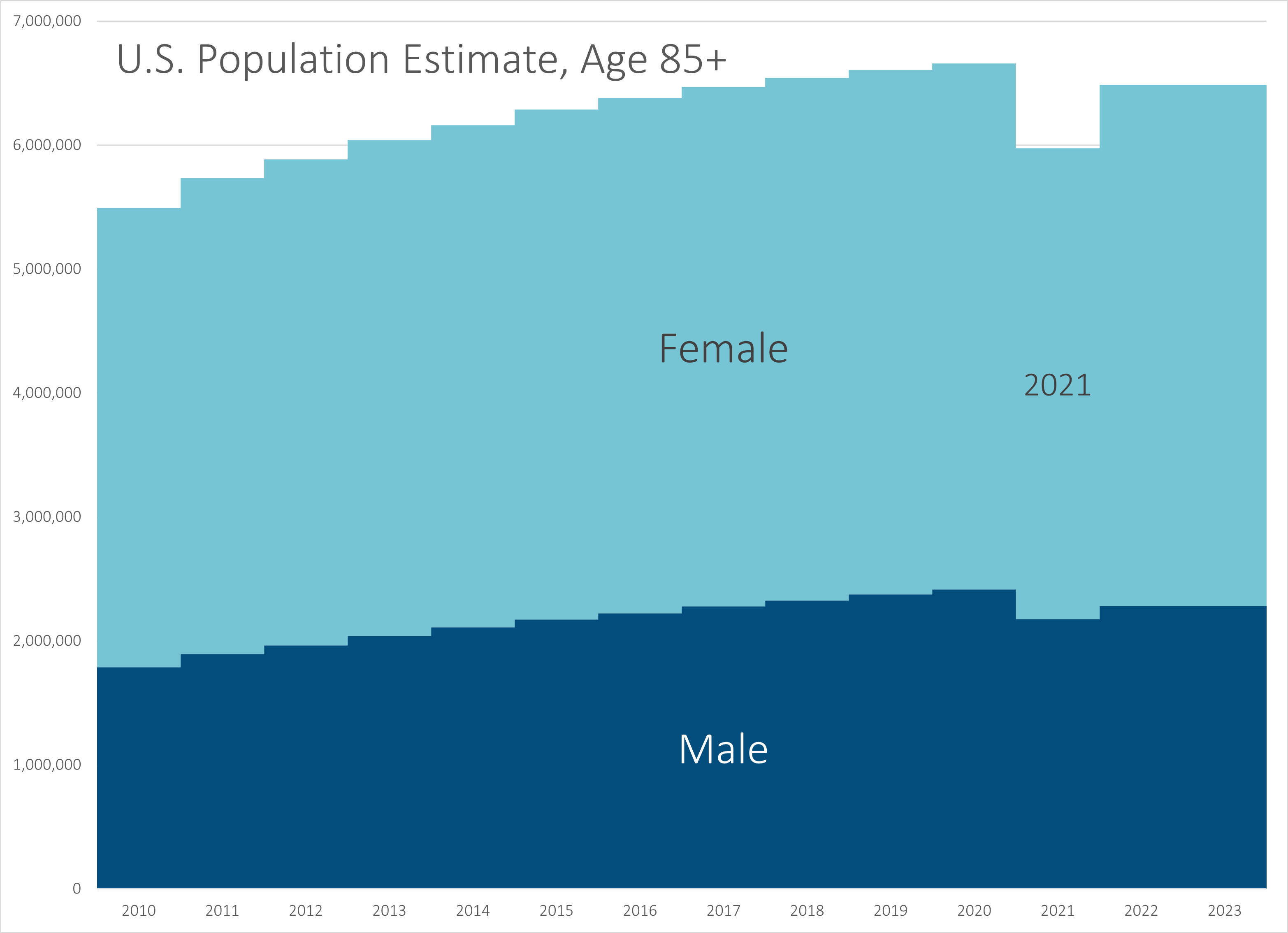
I contacted the CDC WONDER folks, and they confirmed that yes, something was up there.
What is driving this disparity is there’s a “true up” that occurs with each decennial census. The Census Bureau provides the population estimates used in CDC WONDER, and usually this doesn’t cause much trouble.
USUALLY, there isn’t a consequential pandemic occurring when the decennial census enumeration is being taken.
From what I can see, it’s primarily the oldest ages being affected, which is why I had been seeing wonky effects in 2021 (due to timing, one doesn’t see the effects in the census year, but the year after).
I am following up w/ the CDC, as this affects not only what I’m showing you here, but potentially other projects I’m working on (such as reports with the Society of Actuaries).
I believe that the age-adjusted death rates are not greatly affected, given the weights applied to those age ranges:

I have explained about the age-adjusted death rates in the past, but they’re just a weighted average. When the weights are small, any disparities will not have a large effect on the final result.
Increased death rates at younger ages have a much larger effect on age-adjusted death rates than increased death rates at older ages. That is what I have been focusing on lately.
All that said, I may need to update some estimates, but on the whole, many will not change much.
Who is afraid of cancer screening?
I think I will need to return to this, and this “cancer week” has extended into “cancer month” — the Wall Street Journal recently ran this op-ed: Who’s Afraid of Early Cancer Detection?
A diagnosis of pancreatic cancer usually means a quick death—but not for Roger Royse, who was in Stage II of the disease when he got the bad news in July 2022. The five-year relative survival rate for late-stage metastatic pancreatic cancer is 3%—which means that patients are 3% as likely to live five years after their diagnosis as other cancer-free individuals. But if pancreatic cancer is caught before it has spread to other organs, the survival rate is 44%.
The trouble is that this cancer is almost never caught early. There’s no routine screening for it, and symptoms don’t develop until it is advanced. Mr. Royse, 64, had no idea he was sick until he took a blood test called Galleri, produced by the Menlo Park, Calif., startup Grail. He had surgery and chemotherapy and is now cancer-free.
Interjection: Pancreatic cancer was one of the top deadly cancers I noted recently — and unlike the other ones, it had a bad trend:

Early diagnosis is the best defense against most cancers, as President Biden noted when he announced his Cancer Moonshot initiative two years ago. But only a handful of cancers—of the breast, lung, colon and cervix—have screening tests recommended by the U.S. Preventive Services Task Force, an independent panel that evaluates medical screenings.
Many companies are developing blood tests that can detect cancer signals before symptoms occur, and Grail’s is the most advanced. A study found it can identify more than 50 types of cancer 52% of the time and the 12 deadliest cancers in Stages I through III 68% of the time.
There’s a hitch. The test costs $949 and isn’t covered by Medicare or most private insurance. Mr. Royse, a lawyer who works with Silicon Valley startups, paid out of pocket for the test and follow-up imaging to confirm his cancer. Most Americans can’t afford to do so, and some public-health experts think that’s just as well. They fret that widespread use of multicancer early-detection tests would cause healthcare spending to explode. Those fears have snarled Galleri and similar tests in a web of red tape.
There are issues concerning false positives (and false negatives).
Grail’s test has a roughly 0.5% false-positive rate, meaning 1 in 200 patients who don’t have cancer will get a positive signal. Its positive predictive value is 43%, so that of every 100 patients with a positive signal, 43 actually have cancer. That may sound low, but the positive predictive value for some recommended cancer screenings is far lower. Fewer than 1 in 10 women with an abnormal finding on a mammogram are diagnosed with breast cancer.
This is why they keep trying to adjust recommendations for screenings - pushing up the age, or changing the frequency of screenings. If there were a way to pinpoint the people most at risk, and to reduce the number of tests with ambiguous results, the better we would be.
It’s not just a matter of money, but the time and anxiety involved for many would be lessened. I know many women who just want to avoid mammograms because they keep having to go back for more screens.
Here is an opposing view: I Am Afraid of Early Cancer Detection
How about specificity? Let’s consider a fictional, 64-year-old male patient who presents to his internist worried about pancreatic cancer. I pick pancreatic not only because it is a scary cancer: we can’t screen for it, our treatments stink, and it seems to kill half the people in NYT obituary section. I also chose it because it is the anecdotal disease in the WSJ article.
….
Working through the math (prevalence 0.03%, sensitivity 61.9%, specificity 99.5%), this means our patient’s likelihood of having pancreatic cancer after a positive test is only 3.58%. For our patient, we have caused anxiety and the need for an MRI. You almost hope to find pancreatic cancer at this point to be able to say, “Well, it was all worth it.” If the MRI or ERCP is negative, the patient will live with fear and constant monitoring. (You will have to wait until next week to consider with me the impact of this test if we were to deploy it widely).
If the evaluation is positive, and you have managed to diagnose asymptomatic, pancreatic cancer, the likelihood of survival is probably, at best, 50%.
Let’s end this week with two thoughts. First the data for the Galleri test is not good, yet. The test characteristics are certainly not those we would like to see for a screening test. Even more importantly, good test characteristics are just the start. To know that a test is worthwhile, you would like to know that it does more good than harm. This has not even been tested. The WSJ article scoffs at the idea that we would want this data.5
A lot of cancers, we don’t have any way to screen for it — we find out you have it once you’re pretty far advanced in having it. You’re showing symptoms. Some of these cancers (like pancreatic cancer), we don’t have good treatments for.
One hopes the cost of the Galleri Grail test will reduce over time, but the other problems are more difficult to deal with.
I like the fact that you cite dietary differences in regards to life expectancy, "There are a variety of reasons posited for that, but some major reasons can be dietary differences and lower smoking incidence". At my recent PCP visit i was discouraged from loosing more than 5 pounds and my BMI was 29. I am on the way to loosing nutritionally more than that. What is the mathematics of your diet? Prevention remains paramount.