


RIP, Teri Garr: Some Stats on Multiple Sclerosis Mortality
And some of my favorite Teri Garr roles

AP News: Teri Garr, the offbeat comic actor of ‘Young Frankenstein’ and ‘Tootsie,’ has died
Teri Garr, the quirky comedy actor who rose from background dancer in Elvis Presley movies to co-star of such favorites as “Young Frankenstein” and “Tootsie,” has died. She was 79.
Garr died Tuesday of multiple sclerosis “surrounded by family and friends,” said publicist Heidi Schaeffer. Garr battled other health problems in recent years and underwent an operation in January 2007 to repair an aneurysm.
Admirers took to social media in her honor, with writer-director Paul Feig calling her “truly one of my comedy heroes. I couldn’t have loved her more” and screenwriter Cinco Paul saying: “Never the star, but always shining. She made everything she was in better.”
The actor, who was sometimes credited as Terri, Terry or Terry Ann during her long career, seemed destined for show business from her childhood.
Her father was Eddie Garr, a well-known vaudeville comedian; her mother was Phyllis Lind, one of the original high-kicking Rockettes at New York’s Radio City Music Hall. Their daughter began dance lessons at 6 and by 14 was dancing with the San Francisco and Los Angeles ballet companies.
One of my favorite roles of hers was as the spoiled princess in Shelley Duvall’s Faerie Tale Theatre version of The Frog Prince. It was the inaugural episode of this fabulous series of classic tales, with Robin Williams as the title character:
[if this doesn’t cue up at the right point, go to 15:45]
Today: Teri Garr's cause of death explained: 'Subtle' symptoms that led to her diagnosis
Teri Garr, the actor who died Tuesday at 79, was known for her comedic roles, but the star had been dealing with serious health problems for decades.
Garr’s cause of death was complications from multiple sclerosis, her publicist and friend Heidi Schaeffer told NBC News.
She’d also suffered a brain aneurysm in 2006 that left her in a coma for a week.
….
Multiple sclerosis
This nervous system disease affects the brain and spinal cord, leading to damage that affects how the brain communicates with the body, according to the National Library of Medicine.
Women are more likely to get the autoimmune disorder, with warning signs that usually begin between the ages of 20 and 40, the National Institute of Neurological Disorders and Stroke explains.
Garr said she had vague symptoms that started around the time she was filming “Tootsie” in the early 1980s — almost two decades before she was diagnosed.
“I would run, jog in the park, and I just started tripping. It was just like my toe — I would start to trip, and then that would go away. Then I would get some tingling in my arm,” she told CNN’s Larry King in 2002 when she first went public with her condition.
“It’s very hard to get a diagnosis and it’s very hard to find out — difficult to find out if you have this, because the things come and go and the things are subtle.”
She started to walk with a limp and was told she might have an orthopedic problem or a pinched nerve. Garr went to 11 doctors before she was finally diagnosed with multiple sclerosis in 1999, she told Closer Weekly.
The exact cause is a mystery, but genetic susceptibility, infectious disease and environmental factors may trigger the disease, according to The National Multiple Sclerosis Society.
….
People with multiple sclerosis may have double the risk of dying early compared to their healthy peers, a study in Neurology found.
Complications from multiple sclerosis that can lead to death include respiratory and urinary tract–related infection, and aspiration pneumonia from inhaling body fluid or other objects into the lungs, researchers note.
U.S. Multiple Sclerosis Mortality Trends, 1979-2023
Looking at this Neurology study (published 2020)
Abstract:
Objective
To gain a better understanding of the complex patterns of causes that contribute to death due to multiple sclerosis (MS) by assessing the relationship between MS and other causes of death listed on death certificates.
Methods
Multiple cause of death data for all adult deaths (aged ≥18 years) in British Columbia, Canada, between 1986 and 2013 were accessed. All causes, as listed on the death certificate, whether underlying or contributing, were considered “any mention” causes. The associations between mention of MS on the death certificate and mention of other causes of death were examined by logistic regression, adjusted for age, sex, and calendar year (Bonferroni-corrected α level = 0.002). Findings were also sex-stratified.
Results
Among 771,288 deaths, MS was mentioned on 2,153 certificates. If MS was mentioned (versus not mentioned), there was a greater chance that specific conditions contributed to the death: respiratory infection (adjusted odds ratio [aOR], 3.03 [95% confidence interval (CI), 2.73–3.36]), aspiration pneumonia (aOR, 7.15 [95% CI, 6.23–8.22]), urinary tract infection (UTI) (aOR, 10.2 [95% CI, 8.7–12.0]), other infection including sepsis (aOR, 1.34 [95% CI, 1.15–1.56]), and skin disease (aOR, 5.06 [95% CI, 3.96–6.46]). Sex differences existed for urinary tract infection (men: aOR, 14.9 [95% CI, 11.5–19.3]; women: aOR, 8.00 [95% CI, 6.53–9.81]) and chronic respiratory disease (men = aOR, 1.36 [95% CI, 1.14–1.63]; women = aOR, 0.97 [95% CI, 0.84–1.13]).
Conclusions
Deaths attributed to MS were commonly caused by infection (especially respiratory and urinary tract–related); conditions associated with advanced disability and immobility, such as aspiration pneumonia; and chronic respiratory disease in men. All are potentially modifiable; interventions that reduce the frequency or severity of these complications could improve survival in MS.
I’m not going to deal with multiple causes of death (right now), but just looking at MS (ICD-9 code 340; ICD-10 code G35) as the underlying cause of death.
To keep it simple, let’s look at the age-adjusted death rates by sex for 1979-2023.

The jaggedness is an artifact of how the data are given. One gets the age-adjusted rates from CDC WONDER to the nearest tenth (per 100,000 people).
The number of deaths due to multiple sclerosis per year in the U.S. are a few thousand. And there are hundreds of millions of people.
That said, there was a clear increase in the death rates in the 1990s, though primarily for females.

Even given the limitations of that data, there was a clear increase in the death rate for females from MS in the U.S. over those 44 years.
Life expectancy gap for MS patients
2015 paper in Neurology: Effect of comorbidity on mortality in multiple sclerosis
Abstract:
Objective:
We aimed to compare survival in the multiple sclerosis (MS) population with a matched cohort from the general population, and to evaluate the association of comorbidity with survival in both populations.
Methods:
Using population-based administrative data, we identified 5,797 persons with MS and 28,807 controls matched on sex, year of birth, and region. We estimated annual mortality rates. Using Cox proportional hazards regression, we evaluated the association between comorbidity status and mortality, stratifying by birth cohort, and adjusting for sex, socioeconomic status, and region. We compared causes of death between populations.
Results:
Median survival from birth in the MS population was 75.9 years vs 83.4 years in the matched population. MS was associated with a 2-fold increased risk of death (adjusted hazard ratio 2.40; 95% confidence interval: 2.24–2.58). Several comorbidities were associated with increased hazard of death in both populations, including diabetes, ischemic heart disease, depression, anxiety, and chronic lung disease. The magnitude of the associations of mortality with chronic lung disease, diabetes, hypertension, and ischemic heart disease was lower in the MS population than the matched population. The most common causes of death in the MS population were diseases of the nervous system and diseases of the circulatory system. Mortality rates due to infectious diseases and diseases of the respiratory system were higher in the MS population.
Conclusion:
In the MS population, survival remained shorter than expected. Within the MS population, comorbidity was associated with increased mortality risk. However, comorbidity did not preferentially increase mortality risk in the MS population as compared with controls.
To interpret this: it looks like the MS itself didn’t make conditions such as diabetes or heart disease more deadly for MS patients.
The MS itself was what made for shorter lifespans for MS patients.
That said, this was based on a population of almost 6,000 MS patients, and you will notice that in this abstract it doesn’t mention how many total deaths there were in the MS group or the general population group.
Here’s the table:
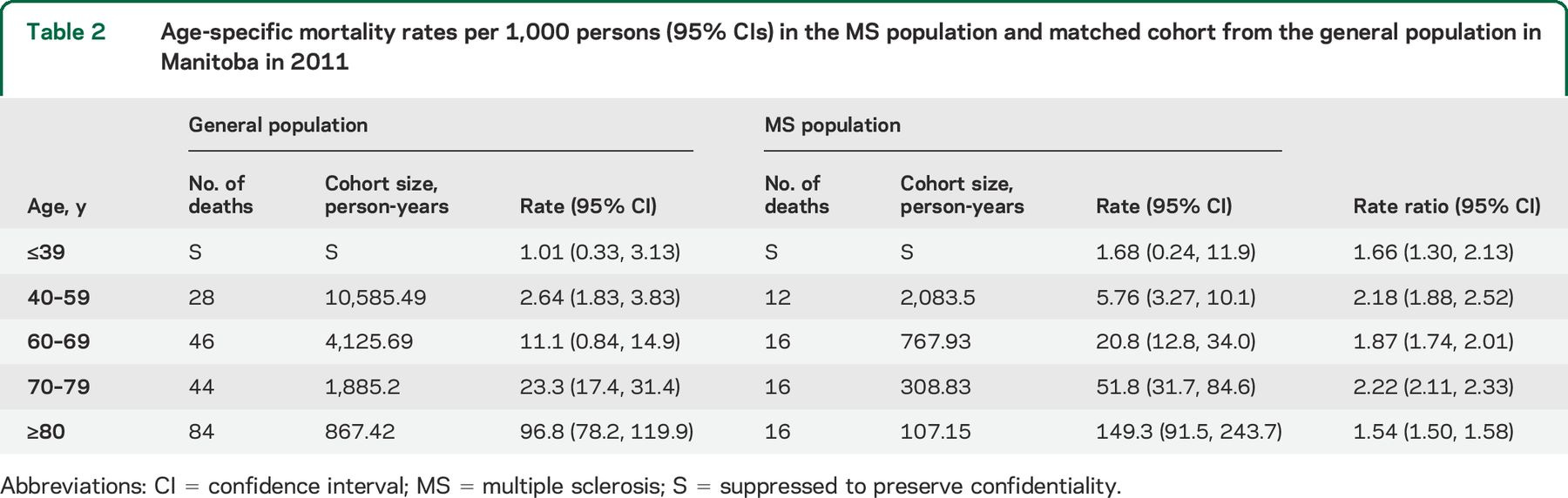
So we don’t know how many deaths are under age 40, but almost certainly it’s under 10. It’s probably extremely few. We will not worry about those.
In the general population group, for those over age 40, there were 202 deaths.
In the MS group, there were 60 deaths.
Notice the confidence intervals they had for their death rates. That gives you an idea of the difficulty many of us have working with death rates. They are actually pretty low, so we generally need very large populations or long periods of time (or a combination) to get a reasonably narrow estimate for death rates.
That said, the rate ratios have narrower ranges.
This is not the only such study showing a gap in life expectancy of about 7 years, though this gap may be shortening:
Disease modifying drugs (DMDs) for relapsing remitting MS only became available in the mid-1990s. Many of the people included in studies used to calculate life expectancy would not have had access to these treatments. DMDs are thought to reduce the risk of inflammatory damage to the brain and spinal cord. So, it is assumed that being on a DMD would slow down the rate at which disability worsens.
In the future, it may be that long-term studies show that life expectancy increases because of these drugs. Indeed, a recent study in Tuscany in Italy suggested that life expectancy of people with MS has improved over the treatment era.
A study published in 2023 that followed people with relapsing remitting MS who had been taking a beta interferon. Taking the drug for more than three years was associated with increased life expectancy.
More effective DMDs have become available. So, the gap between people with MS and the general population will hopefully close further and the extra years of life will be of a higher quality.
In many cases, the life expectancy gap persists, but life expectancy has improved for the general population and the MS patient population concurrently:
A Norwegian study found that life expectancy in people with MS is increasing at the same rate as that seen in the general population. Overall, life expectancy was seven years less than people who didn't have MS (74.7 years vs 81.8 years).
It’s a bit difficult to make up the gap while the overall population is also improving.
That said, most people who are diagnosed with MS are diagnosed in younger adulthood, and live with the condition for decades. Most have an intermittent version for a while, before it becomes persistent and progressive in terms of disability.
Teri Garr and Posthumous Obits
In the case of Teri Garr, she was diagnosed in 1999, so she outlived her diagnosis by about 25 years.
But what’s interesting to me is that she outlived her obituary writer:
Bob Thomas, a longtime Associated Press journalist who died in 2014, was the principal writer of this obituary.
To be sure, for famous people, the obits are mostly pre-written. In the case of Teri Garr, who had a severe health event in 2006 (aneurysm and then coma) and had to retire due to that, I imagine they had one written for her by 2007.
The above piece is from 2005 and re-posted by CBS yesterday.
Another of my favorite roles of hers was in Mr. Mom, a movie I enjoyed when I was a little kid. I liked the bit where she did the pitch on the tuna ad:
Even as a kid, I liked the business pitch.
RIP, Teri Garr.
Great clip - I love this bleeding heart shit, too! Thought she was brilliant in Young Frankenstein. On MS, my understanding is that incidence varies widely by state or at least geography, with a lot of cases, for example, in the northern Midwest. I think I read once there aren't many cases down South. I knew several people who had MS when I lived in MI, and virtually no one from anywhere else (I've also lived in the Northeast). Anecdotal, of course, but it was striking to me.