


Covid Round-up: The Case of the Mysterious Missing Mortality and More
Also: not-so-missing mortality

Again, as the Actuarial Outpost is in a weird situation right now, stories that I would normally add to the AO’s ginormous COVID thread, I’ll put on the blog.
[For the record, it looks like the old version of the Actuarial Outpost will disappear, with the new one being something I’m unlikely to be involved with.]
Case Surges, With and Without Excess Mortality
Some really weird things are going on, which is a reminder that even if you think you know what underlies the data… you probably don’t know what underlies the data.
Illinois will never get back to any sense of normalcy as long as the media and Gov. J.B. Pritzker continue to push cases as the key measure of the virus’ danger to the general public. As we wrote last month, it’s not cases that matter, but hospitalizations and deaths.
That’s important because there’s been no real increase in hospitalizations or deaths for three whole months. Cases have tripled since their lows on June 18, yet the average daily death rate has actually fallen from 50 then, to about 19 today.
We’ve heard no explanation from Pritzker and others on why hospitalizations and deaths haven’t increased. Instead, they continue to treat case growth and positivity rates as what really matters.
I can think of all sorts of explanations, but the Wirepoints guys basically have the same ones as me:
Here are a few of the questions the governor should answer: Are cases way up and hospitalizations flat because it’s young, healthier people that make up most of the new cases? Is it because there are many more asymptomatic cases? Is it because newer cases are coupled with fewer pre-existing conditions? Is it because the virus has already spread through Illinois’ most-vulnerable populations? Is it because Illinois is finally protecting retirement home residents better?
We can’t answer any of the above questions because Gov. Pritzker and the Illinois Department of Public Health won’t provide such data. And it’s not like they can’t. Other states do.
The example they give is Florida, which does give info by age and co-morbidities. The Illinois death data graph is bullshit (it’s by reported date of death, not occurrence of death), but hospitalization data is good:
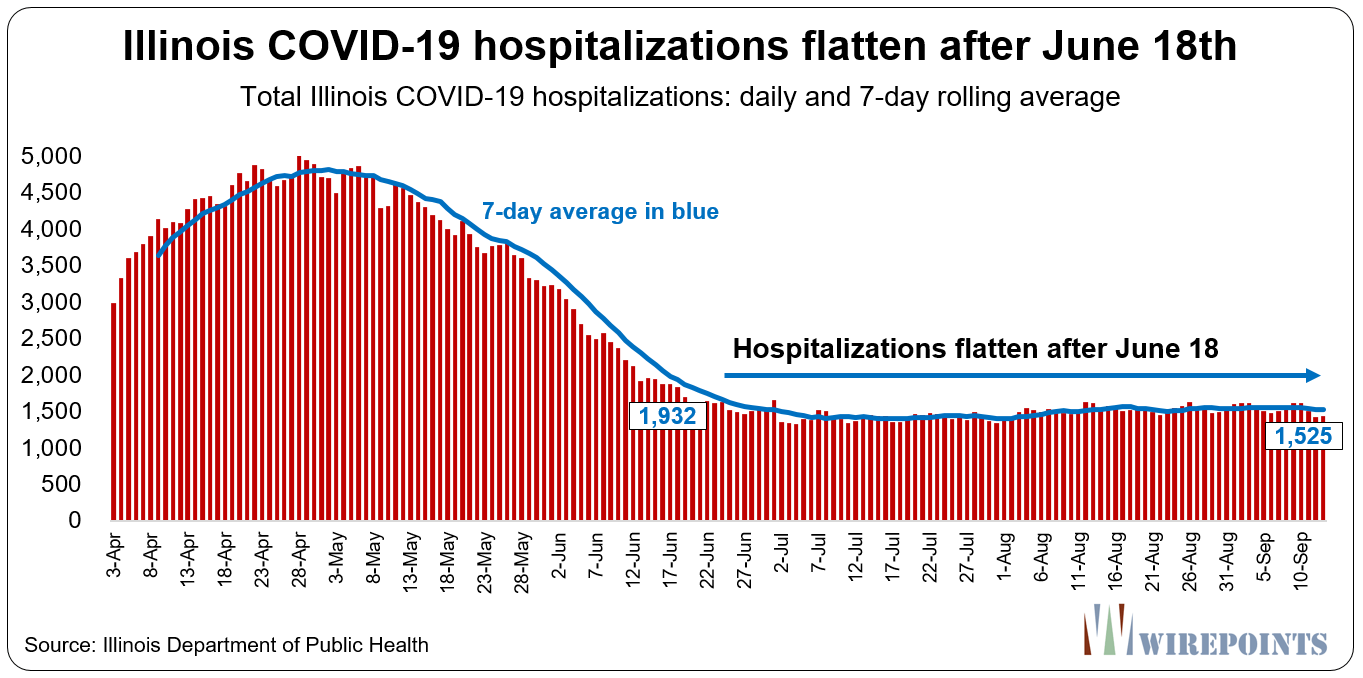
You don’t even need to do the 7-day rolling average with that data. It’s in a steady-state condition, looks like. Hmmm.
Anyway, Illinois is not the only place reporting a huge increase in COVID cases, but no increase in deaths or hospitalizations. Sure is weird.
Something similar is going on in Europe:





(Again, you see the idiocy of death & case by reported date, as opposed to incurred date or tested date) Tom Gara noted these stark contrasts.
You can see for yourself: cases increasing, and deaths… barely increasing. I think a big difference is, of course, the availability of testing in the first wave. Current testing is definitely catching people who would not have qualified to get tested when tests had to be rationed.
Andrew Sullivan points out that Africa seems to be completely bypassed by COVID, though it seems there were infections. The following is from Science magazine:
After testing more than 3000 blood donors, Uyoga and colleagues estimated in a preprint last month that one in 20 Kenyans aged 15 to 64—or 1.6 million people—has antibodies to SARS-CoV-2, an indication of past infection. That would put Kenya on a par with Spain in mid-May when that country was descending from its coronavirus peak and had 27,000 official COVID-19 deaths. Kenya’s official toll stood at 100 when the study ended. And Kenya’s hospitals are not reporting huge numbers of people with COVID-19 symptoms.
Other antibody studies in Africa have yielded similarly surprising findings. From a survey of 500 asymptomatic health care workers in Blantyre, Malawi, immunologist Kondwani Jambo of the Malawi–Liverpool Wellcome Trust Clinical Research Programme and colleagues concluded that up to 12.3% of them had been exposed to the coronavirus. Based on those findings and mortality ratios for COVID-19 elsewhere, they estimated that the reported number of deaths in Blantyre at the time, 17, was eight times lower than expected.
Sullivan’s point is this:
We know less about this virus than we sometimes think we do. And if someone comes along and tells you there is a simple, single, ideological explanation for all its demographic impacts, retain a modicum of skepticism.
He has a political point to make, but I have a more general point to make: a lot of people have tried to exude knowledge with respect to this pandemic, and pretending that you know anything solid is fatuous.
When I noticed the August case surges, but lack of excess mortality in some places [but others did show excess mortality], I heard the “wait two more weeks” bullshit as from before. The cases took off in August… the extra deaths should have already shown up by now.
Quick break for Mortality with Meep Video
And by “quick”, yeah, it’s about 20 minutes. I look at the CDC total deaths information, which is by week, and was updated to 18 September 2020 at the time I recorded it.
Video: Excess Deaths in U S – CDC Views – September 2020 update
More on European COVID surges
BBC: Coronavirus: WHO warns Europe over ‘very serious’ Covid surge
Speaking in Copenhagen on Thursday, Mr Kluge said 300,000 new infections were reported across Europe last week alone and weekly cases had exceeded those reported during the first peak in March.
“Although these numbers reflect more comprehensive testing, it also shows alarming rates of transmission across the region,” he told reporters.
…..
Hospital admissions and deaths have not yet seen a similar rise, although Spain and France are seeing an upward trend.While younger people – who are less likely to be severely impacted if they are infected – currently make up the largest proportion of newly recorded coronavirus cases, there are fears of many more cases of serious illness if the virus spreads to older and more vulnerable groups.
Maybe you guys already had your sweep through the old folks… or the old folks know how to stay away from young spreaders now.
Reuters: Second UK lockdown? England COVID-19 cases rising by 6,000 per day
Britain was on Friday considering whether to impose a second national lockdown, after new COVID-19 cases almost doubled to 6,000 per day, hospital admissions rose and infection rates soared across parts of northern England and London.
The United Kingdom has reported the fifth largest number of deaths from COVID-19 in the world, after the United States, Brazil, India and Mexico, according to data collected by Johns Hopkins University of Medicine.
Reminder where these nations land in countries by population
United States: 3 (330 mil)
Brazil: 6 (211 mil)
India: 2 (1,366 mil)
Mexico: 10 (128 mil)
UK: 21 (68 mil)
It’s good to do proper comparisons.
Its model pointed to about 6,000 new cases a day in England in the week to Sept. 10, up from 3,200 cases per day in the previous week, with the North West and London seen as hotspots.
“There is evidence of higher infection rates in the North West and London,” the ONS said.
As those figures were published, Britain imposed new COVID regulations on the North West, Midlands and West Yorkshire from Tuesday. Countries around the world where COVID-19 cases are on the rise are similarly tightening rules, and Israel on Friday announced a second nationwide lockdown.
…..
On Thursday, Britain recorded 21 deaths from the disease, taking the total under the government’s accounting method to 41,705. Key statistics on the prevalence of the virus are due later on Friday.
More than one-seventh of the UK population is in local lockdown.
Excess mortality isn’t just COVID deaths
I am still very suspicious of Alzheimer’s death spikes from April.
WSJ: Death Toll From Covid-19 Pandemic Extends Far Beyond Virus Victims
From Alzheimer’s disease deaths to fatal heart attacks, federal data show deaths in 2020 have exceeded those of previous years in numerous categories. Doctors and health researchers say the fatalities reflect the ways the pandemic has amplified stress and financial strain while causing many people to avoid hospitals for fear of infections.
…..
Some of these additional deaths were probably caused by Covid-19 but not recorded as such on death certificates, but others likely represent indirect fallout from the pandemic, said Robert Anderson, chief of the mortality-statistics branch at the CDC’s National Center for Health Statistics. “We had no experience with this sort of thing, really,” Mr. Anderson said, regarding the pandemic. “The more we can learn about how things played out here and how the virus impacted mortality — not just directly, but indirectly — can help us God forbid we have another one of these.”The CDC estimates there were somewhere between about 202,000 and 263,000 excess deaths in the U.S. this year through late August, measured against deaths from 2017 through 2019. The U.S. by that point had about 188,000 known Covid-19 deaths, according to Johns Hopkins. In New York City, the citywide death count surged by 35,000 in the most recent fiscal year, far exceeding the 19,142 confirmed and 4,625 probable virus-related deaths, authorities said Thursday.
Researchers are still trying to understand these gaps between total pandemic-related deaths and those caused by coronavirus infections, including how many actual Covid-19 deaths were undercounted. This could take years to unpack as scientists learn more about Covid-19 and wade through inconsistencies in how death certificates are filled out. Researchers say there may also some lockdown effects that improved health, such as reduced air pollution.
Blah.
General COVID and mortality-related stories
Slate: Racism Is a Pandemic: We need to treat it like the same public health emergency that COVID is. I have mentioned the racial gap in U.S. mortality before. It’s swamped by the sex gap in mortality:

Note that black women have a life expectancy two years higher than that of non-Hispanic white men. Clearly, sexism is killing men.
Or, perhaps, the dynamics are not that straightforward. I will not doubt that both racism and sexism were far worse a century ago, during the Spanish flu pandemic.
And yet, African-American mortality during the Spanish flu was lower than white mortality:
Contradicting prevailing theories about African Americans’ increased susceptibility to disease, it appears that during the 1918 epidemic the incidence of influenza was lower in African Americans. Although the epidemic had a less devastating impact on African American communities, it still overwhelmed their medical and public health resources.
…..
Black physicians contended that it was a “matter of common observation” by physicians and the lay public that the “susceptibility and fatality” during the epidemic had been greatest among whites.”77 A January 1919 editorial in the Journal of the National Medical Association pointed to data from the Philadelphia Board of Health that showed that between September 20 and November 8, 11,875 white people died from influenza and pneumonia and 812 black people died. The editorial called the racial differences “interesting” because the death rates of African Americans in the city were “normally much higher than that of the white.”78
I have looked up historical mortality tables by race, and the racial mortality gap between black & white used to be much worse than currently. From a CDC study. In 1900, the difference was almost 15 years – a lot of that driven by infant and child mortality, as life expectancy for both whites and blacks was under 50. But we can look at those stats another time.
Others without comment:
WSJ:In Brazil, Covid-19 Deals New Blow to Children Disabled by Zika
WSJ: The Worst Month for U.S. Traffic Deaths – There is a COVID connection: “Not only are we getting into September, which is associated with higher-risk travel, but we’re also rebounding from Covid-19 lockdown measures,” [Samuel Monfort, statistician with the Insurance Institute] said. “We might not see the drop in vehicle miles traveled that normally happens around this time. It’s something people should be aware of and maybe drive more carefully.”
Gizmodo: Should a Covid-19 Vaccine Be Mandatory for Kids? Health Experts Are Trying to Decide
WSJ: Covid-19 Test Maker Examines False-Positive Results in Nursing Homes
Nature: Researchers highlight ‘questionable’ data in Russian coronavirus vaccine trial results
Americans’ Poor Health Paved The Way For Covid Deaths – (I think this is overblown; U.S. COVID deaths are primarily old folks. Complaining that the 85+ year olds aren’t in great health…..come on)
WSJ: What It Would Take for Herd Immunity to Stop the Coronavirus Pandemic – this is also with a vaccine. Measles requires over 90% community immunity, which is mainly through vaccines right now, for example. For COVID, they assume the natural infectiousness requires only 60 – 70%.
The Verge: Why it’s important to look for the limitations in coronavirus studies
The Atlantic: How We Survive the Winter
PoliMath: Every State’s COVID Numbers in Context, September Edition
Reason: Can the CDC Get Anything Right?
Enjoy!