


COVID round-up: Reduced deadliness, length of immunity, second (and third) waves, and more
Back to reality

The Actuarial Outpost, as it was, is finally dead. For actuarial chatter, join us at Go Actuary.
For those who used to keep up with my “watch” threads, I will be sharing the links on my blogs for now. I’m looking for a content management solution for what I want to do with that stuff. (I prefer my memory to be external to me and my computers.) It may end up being Wordpress by default (my webhosting company provides this), but if anybody has better options, please email me (marypat.campbell@gmail.com) or tweet at me (@meepbobeep).
This is a COVID news round-up thread. The death-rate-based sequel to my post on total death numbers and pandemics will be coming later.
Evidence of reduced deadliness in subsequent COVID waves
Let’s start with good news.
WSJ, 22 October: New York City’s Covid-19 Death Rate Has Dropped in Recent Months
New York City residents are dying at a lower rate from the coronavirus than at the height of the pandemic in the state, new research shows, but doctors haven’t been able to fully explain the reason for the drop.
The findings, released Wednesday by NYU Grossman School of Medicine and published in the Journal of Hospital Medicine, show that regional death rates of hospitalized patients have dropped from highs in the spring when New York City hospitals were at capacity and hundreds of New Yorkers were dying daily.
Hospital data drawn from the NYU Langone Health system from March through August show that out of 5,121 patients hospitalized with Covid-19, mortality rates dropped to 7.6% in August from 25.6% in March.The data show that even after accounting for patient demographic and clinical factors, mortality from Covid-19 is decreasing, researchers said. But they can’t pinpoint why, said Leora Horwitz, the study’s lead author and an associate professor in the Department of Population Health at NYU Langone.
Researchers said patients were arriving at hospitals with less-severe symptoms. Beyond that, said Dr. Horwitz, lower death rates are likely a combination of better medical treatment and better understanding of the disease by doctors.
Here is the press release from NYU: Study Helps Explain Declines in Death Rates from COVID-19
Fewer New Yorkers are dying from 2019 coronavirus disease (COVID-19) than health experts had anticipated, a new study shows. Regional death rates have dropped from the highs seen at the start of the outbreak, partially due to a shift in the population contracting the disease toward those who are more resilient.
…..
Instead, a new investigation showed that by mid-August, the death rate in those hospitalized with coronavirus-related illness had dropped from 25.6 percentage points to about 7.6 percentage points. Led by researchers at NYU Grossman School of Medicine, the study showed that a younger, healthier group of people were getting infected and were arriving at the hospital with less severe symptoms than those infected in the spring.However, the researchers’ analysis showed that these factors accounted for only part of the improvement in survival. The rest, they suspect, resulted from healthcare providers’ growing experience with the coronavirus. For example, physicians learned that resting COVID-19 patients on their stomachs rather than their backs and delaying the use of ventilators as long as possible were more effective practices, say the study authors. Drugs likely helped as well. In addition, other factors such as decreasing hospital volumes, less exposure to infection, and earlier testing and treatment, may have played a role.
Okay, so the people getting infected now aren’t the captive residents of nursing homes, but younger people who have been out & about.
The average age of hospitalized COVID-19 patients also dropped from 63 to 49. In March, while 81 percent had chronic conditions like lung disease and diabetes, by mid-June only about 72 percent had such risk factors.
Here is a link to the academic article: Trends in COVID-19 Risk-Adjusted Mortality Rates
And I just want to show a graph from the study:
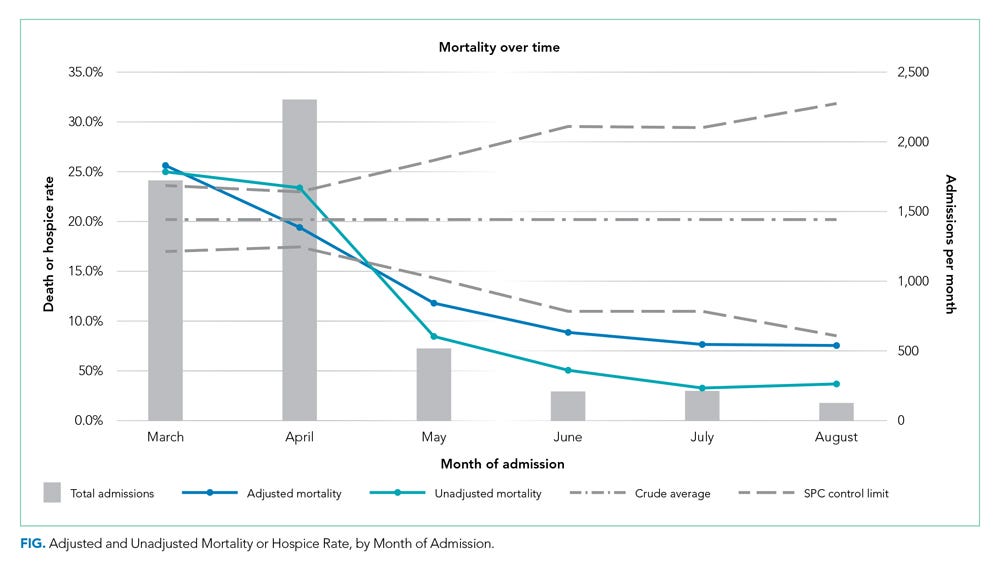
And this text:
Similar risk-adjusted results have been preliminarily reported among intensive care unit patients in a preprint from the United Kingdom.9 Incremental improvements in outcomes are likely a combination of increasing clinical experience, decreasing hospital volume, growing use of new pharmacologic treatments (such as systemic corticosteroids,10 remdesivir,11 and anticytokine treatments), nonpharmacologic treatments (such as placing the patient in the prone position, or proning, rather than on their back), earlier intervention, community awareness, and, potentially, lower viral load exposure from increased mask wearing and social distancing.12
Maybe there’s better treatment in general… maybe they burnt through their “dry timber” of old folks in nursing homes.
More items on a similar theme:
The New Neo: COVID death rates continue to fall
Transboundary and Emerging Diseases, September 6: Decreased Case Fatality Rate of COVID‐19 in the Second Wave: A study in 53 countries or regions
WaPo, Oct 9: Covid-19 death rates are lower worldwide, but no one is sure whether that’s a blip or a trend
COVID immunity might not last
So here’s the bad news.
WSJ: Study Shows Covid-19 Antibodies Waning Over Time, Suggesting Immunity Might Wear Off
LONDON — A large English study showed the number of people with Covid-19 antibodies declined significantly over the summer, suggesting that getting the virus might not confer long-lasting immunity from future infection.
The survey of 365,000 adults in England who tested themselves at home using a finger-prick test showed the proportion of people testing positive for Covid-19 antibodies declined by 26.5% between June 20 — 12 weeks after the peak of infections in the country — and Sept. 28.
The results also suggested that people who didn’t display symptoms were likely to lose detectable antibodies before those who had showed symptoms. The study, conducted by Imperial College London and the Ipsos Mori polling organization, was funded by the British government, which announced the results and published the study on Monday night. The results haven’t yet been reviewed by other experts.
Doctors don’t yet know whether antibodies confer any effective immunity against reinfection by Covid-19. But even if they do and the results of this survey are confirmed, it suggests the prospect of widespread long-term herd immunity to the virus will be difficult to achieve. Herd immunity occurs when enough people in a population develop an immune response, either through previous infection or vaccination, so that the virus can’t spread easily and even those who aren’t immune have protection.
The findings showed 18- to 24-year-olds lost antibodies at a slower rate than those aged 75 and over. The smallest decline of 14.9% was of people aged between 18 and 24, and the largest decline of 29% was of people aged 75 and over.
So just a few comments – and remember, the following is just about possibilities and not even probabilities.
But I want you to think about the flu and colds. These are caused by viruses. You can get a flu shot that’s actually a good mix for a year and still get the flu; there is no shot for colds. People have been dying from the flu, and pneumonia stemming from the flu or colds, in tens of thousands in the U.S. every year for many years.
COVID may end up part of the disease mix we have to deal with year-after-year. It may be like flu, with annual shots, with varying levels of efficacy. There may be no effective shots whatsoever, as with colds. `It may be like measles or diphtheria, where we can make a vaccine close to 100% effective. We don’t know yet.
Related:
CNN: British study shows evidence of waning immunity to Covid-19
Nature: Why decoding the immune response to COVID matters for vaccines
Nature: How obesity could create problems for a COVID vaccine
NYT: Some Covid Survivors Have Antibodies That Attack the Body, not Virus
Reuters: UK study finds evidence of waning antibody immunity to COVID-19 over time
NPR: Eli Lilly Ends Antibody Trial In Hospitalized COVID-19 Patients, Other Trials Go On
Reality check: you can’t always get what you want
Many people, especially policymakers, need to realize what is within the range of possibility, and what actually can and cannot be practically controlled.
If you say that you’re not going to do XYZ until there’s a 95% effective vaccine (or whatever), are you willing to not do XYZ for 10 years? Longer?
Maybe there will be a vaccine at your preferred confidence level within a year, and maybe… there will not be. And such a vaccine may never come.
When it’s individuals making choices for themselves, some things are easy to say, “We won’t”. There are certain things that Stu & I will not do, indefinitely, because of his cancer and his vulnerabilities. That predates COVID-19. We’ve weighed the risks and benefits, and there are lots of group activities I just have to forgo, because I’m not risking spreading COVID to Stu so I can entertain myself. This is something I can extend indefinitely.
Stu and I can lock ourselves down from outside supplies for a certain amount of time, but there is a limit to how long we can go without contact with the outside world, at least in the form of food and other supplies. So we have some practical limits to what we can put up with.
Then there are the policymakers. They’re ostensibly making decisions for other people, and many of their public pronouncements have been absurd, as they’re predicated on certain conditions which may never obtain.
Some pronouncements they could get away with for a few months. Not for a decade. Heck, not even a full year, for many of the proclaimed policies.
WSJ, October 26: Pandemic Fatigue Is Real—And It’s Spreading
From the corridors of Washington to the cobblestones of Paris, the coronavirus is roaring back and authorities are ramping up restrictions again. This time around, however, everyone is tired.
Hospital staffs world-wide are demoralized after seven months of triage. The wartime rhetoric that world leaders initially used to rally support is gone. Family members who willingly sealed themselves off during spring lockdowns are suddenly finding it hard to resist the urge to reunite.
….
Too much pandemic fatigue, authorities said, can fuel a vicious cycle: A tired public tends to let its guard down, triggering more infections and restrictions that in turn compound the fatigue. That is part of what is driving the recent spate of policy reversals. Bars and cafes that reopened after the spring lockdown are off-limits again.Workers who were told to return to their offices are being asked to work from home if possible. In France, authorities recently halved the length of quarantines to one week, believing it would boost compliance.
“It’s a matter of balance. To be able to enforce a new rule, we need to make sure first that people can accept it,” Education Minister Jean-Michel Blanquer of France said.
I could make this political, but no, this is not really about politics as you may normally think it.
This is about how humans actually behave.
Plague and pandemic are not new to human civilization
I will never stop flogging this — I highly recommend reading Daniel Defoe’s A Journal of the Plague Year, about the last huge and deadly plague outbreak in London, in 1665 (which then got followed by the Great Fire of 1666 – so hold off on your 2020 jokes… yes, it can get much, much worse than what we’ve already seen).
This book has been misclassified as a novel by some, because he puts some narrative into it (and yes, some is of a friend-of-a-friend nature that obviously did not happen, and, being an honest journalist, Defoe points that out). It really is a nonfiction book based on government records, official history, and Defoe capturing stories survivors told of the plague that year (he was a little kid in 1665, and the book was written decades later. The core “story” is probably from the point-of-view of Defoe’s uncle.)
I made a video on March 25 about this book, and in the video notes I mention: “I highly recommend pandemic policy-makers to read Daniel Defoe’s classic (from 1722) A Journal of the Plague Year, which is more nonfiction than fiction”.
I was not being snide or flip in that recommendation, which was well before the most idiotic of the policy-making of this year. What Defoe had to write about poor decisions made by London officials at the time applies today. Defoe’s insights were not unique, as other plague/pandemic accounts attest, but he was the best nonfiction writer who put these issues down in text.
[I swear, I want to publish an annotated version of his book – maybe there can be a graphic novel version to make it even easier for politicians.]
There are limits which even the most authoritarian/totalitarian governments can’t get past… because people are people (and so are the components of their government). You can’t shift blame to models or algorithms – they can’t take the blame. The humans who built them can be blamed, as can be the humans who tried to shift “decision-making” to these tools.
If you don’t understand how humans are likely going to behave… you should not be setting any sort of policy. Just go do something else. It’s a large world and many things to do in it. Sometimes, they also serve who stand and wait.
My post referring to Defoe’s book..
More on the same theme from Polimath: Watching A Wave Come In
COVID waves around the world
The Economist (free to read): The second wave in Britain
Although britain’s covid-19 death numbers are nowhere near their spring peak, they are climbing dangerously. Daily tolls are similar to mid-March. Things are particularly bad in the north. Field hospitals in Harrogate, Manchester and Sunderland are on standby. Under a new regime of regional lockdowns which went into effect on October 14th (see map), gyms, bars and casinos in Liverpool will be closed, and non-essential travel in and out of the area discouraged. In much of northern England and part of the Midlands, members of different families will not be able to meet indoors, and the use of public transport will be discouraged; London is expected to be put under the same restrictions shortly.
Britain can probably withstand a second wave better than the first. It has the capacity to perform 13 times as many tests each day as in mid-April. Deaths and hospitalisations are rising more slowly than they were in the spring. Doctors now know to place patients on their stomachs, to delay ventilator use and what drugs to use. There is plenty of protective kit for health-care workers, and the nation has got used to wearing masks and working from home.
I am not trying to belittle these second waves of cases — they do reflect real, recent increases. The increased volume of testing is capturing something real, because low case numbers also came with that increased volume, at least initially.
What is silly is trying to compare current case numbers with spring case numbers. The increased volume in testing 6 months apart makes a huge difference.
Other waves:
Naked Capitalism: Covid Spikes in Europe, US Before Winter Is Here
Axios: Putin mandates face masks as Russia combats second COVID-19 wave
NYT: Hospitals Are Reeling Under a 46 Percent Spike in Covid-19 Patients
The Economist mortality tracker
The Economist: Tracking covid-19 excess deaths across countries
This is a good interface, with sparklines and more. Eyeballing it, the U.S. numbers look like they’re straight out of the CDC, and I like the current “heat map” they have at the top – you can see many, like the U.S., report total deaths by the week, but some countries only have numbers by the month. You can really see the mortality waves, and I wish they’d re-order the countries so you can see the wave hit Italy and then Spain, etc. It looks like they’ve ordered the heatmap by total mortality, kind of, but I still think they could re-order for better display. This page was originally published in July and they keep updating it, so perhaps it will give you a better display by the time you click through.
There are loads of breakdowns: by age (in Europe), by areas of countries that have that info. All their data is on github. I will likely be looking at it later for the European data sets, as I’m fine with the CDC setup for grabbing the data for the U.S.
COVID links
Some of these aren’t COVID-specific, or even recent, but came up in my past week of reading.
Plague transmission rates increased from the Black Death to the Great Plague – that’s the 1348 to 1666 (in England)
PoliMath: Every State’s COVID Numbers in Context, October Edition
WSJ: ‘If Anything Happens to Me…’ Inside One of America’s Worst-Hit Nursing Homes
NYT: How the Coronavirus Compares With 100 Years of Deadly Events
The Zvi: Covid 10/15: Playtime is Over and Covid 10/22: Europe in Crisis
UK Spectator: The ten worst Covid data failures – these are all UK disasters, including the Excel screw-up, but a few of these apply to the U.S. broadly, as well. In particular: “Reluctance to acknowledge uncertainties in evidence” – I have been ranting about this one in particular, and have deleted about half the things I start writing about it, as one shouldn’t blog angry.
CDC reports 300K more deaths than expected this year, likely due to COVID-19
On spreadsheet screw-up on testing: Don’t blame software for missing tests – it’s down to a lack of basic data handling skills
American Journal of Public Health, May 2020: Fifty Years of Influenza A(H3N2) Following the Pandemic of 1968
Marketwatch, July 2020: Here’s one ‘remarkable’ difference between COVID-19 and the 1918 Spanish flu
The Economist free to read: The pandemic is plunging millions back into extreme poverty
Hospital Admissions Statistics – A fair representation of the true position? — this is from a UK actuarial group, with more bulletins here
VoxEU: Trust and compliance with public health policies in the time of COVID-19
Reason: A New Study Estimates That COVID-19 Is Responsible for 2.5 Million Years of Life Lost in the U.S.
Governing: With COVID Cases Rising, What Policymakers Need to Know
COVID’s cognitive costs? Some patients’ brains may age 10 years
Study finds over 80 percent of COVID-19 patients have vitamin D deficiency
The Economist (free-to-read): China calls its “heroic” handling of covid-19 proof of its wisdom
Don’t assume the Economist is simply parroting the CCP line in that piece:
Yet a core claim made by the party is also false—that its crushing of covid-19 proves the unique advantages of autocracy. Off China’s coast, the democratic island of Taiwan has handled the virus brilliantly, recording just seven deaths in a population of 23m.
Entire continents have had very different COVID results, and it may be good to think about what may actually be going on in Asia vs. Africa vs. Europe vs. the Americas.
We still have huge gaps in our knowledge about COVID, and it is good to realize that it will take some time to understand better.